
Premium workshop
You can view a 2 minute preview. For details, scroll down below the video.
Description
Objectives
- Learn the differences between the anatomical and functional definitions of fascia
- Learn how fascia therapy can be used to help with pain in some people
- Learn how to assess body types and then what exercises are most beneficial
About This Video
Transcript
Read Full Transcript
Chapter 1
Trailer
Hello, I'm Robert Fly. I'm, I'm proud and happy to present to you this new lecture on Fascia and Davis Law. It will have three parts. The first is the summary of the latest insights from the last two years. That includes the different layers of the lumber Fascia, three different layers. It also includes uh, how fashion responds to different kinds of loading and also many other more recent insights.
Then in the middle parts we will come to David's law that states that faculties use respond to different loading with very different architectural responses. And in the last part of this lecture, I will show you three different tests to find out what your genetic constitution you may have. Some of you are more equipped for r y king, like sturdy body, but others are more like a bendy Wendy person who is hyper mobile everywhere. And finally a third type, which is not so much genetic, but it's driven by our subtle society. It's based on Vladimir Yonda, the crossover type. So applying this to your daily practice can be very useful, not only based on these tests, but if we take these tests and you have somebody who you'll find out is more y king person or hyper mobile person, you will design your exercises very different.
So I think everybody can profit from this course. First of all, the information is the latest insight. And no matter how smart you are, I promise you will find some new information that you will feel are gold mines by itself, but also fresh beginners. Yuval have a lot of new insights that really make sense. You will go out with a sense of Aha, they are, I have a new direction, how I can help this person, how I can design my exercises different and also new ways of asking new questions. Thank you very much. Uh,
Chapter 2
Anatomical and Functional Definitions of Fascia
I'm very honored to be here this third time now and take a very much for Christie, for inviting me in. I see some familiar faces here. So in this lecture I will give new information in relationship to Fascia, how it we late for movement professionals in first a interest for Pilatos instructors but also for yoga instructors, fitness instructors, athletic trainers, dancers, dance teachers, et Cetera. From my background, I've been a bodywork instructor for almost three decades.
And then I tried the field of academic science and I found that very, very fascinating. And in the last few years, a lot of new things have happened in the field of academic factual research where many of us had a sense this has a lot of practical value for people. We're working with a more holistic attitude in the human body. So in this lecture I will focus on Fascia and the so called Davis Law. And my hope is that the Davis law will be new to you. So you will learn something new in this lecture.
It will build on a Fascia and Fascia science lecture that I have been giving here two years ago. So in the first part of this lecture it will have three parts. Uh, I will cover what new information in Fascia research internationally, uh, has been happening in the last two years since the last fashion science lecture that I've been giving here for Pilatos anytime that is relevant for movement instructors. And then I will focus on this Davis law that describes how collagenous connective tissue adapts to training and to loading to overloading, to under usage and to appropriate loading. And where are the different thresholds. This is new and very fascinating and very relevant information.
And once we have covered that in the last portion of this lecture I will introduce three mobility tests. How you can find out whether you have a genetic constitution for increased mobility or hypomobility in some of them, no matter which joint you are looking at or whether you are more what we call a viking person who is equipped. There's a lot of stability but has to work hard to stay flexible at their different joints. And I will also then introduce a certain typology, the crossed over technology based on Vladimir Uganda where you have some joints where you are hyper mobile and other points where you are more stiff. So these are the three parts of the lecture. So let me get started and also at the very end I hope to get questions from you and that usually is the most interesting part.
If you have any questions in between, I'm willing to jump on them and take them, uh, for the benefits of all. So, uh, an important thing that has happening in the field of Asher research is that we had an ongoing debate what tissues can you include to call Fascia. And there was a couple of months ago the last international Fascia Research Congress and finally there was some agreement that from now on we will be using two different fasher terms. One that is more specific for communicating with medical professionals and when you are looking at small pieces of the human body and they are, we decided to align ourselves not so much with Grey's anatomy. For some of you, Grey's anatomy is quite familiar because it's the most authoritative book out there, but more with the International Federated Committee on anatomical terminology that was based not only on political reasons but also because they seem to get their stuff together to come up with a new international medical terminology in this year 2016 and they actually reached out to us to help them with their many different Fascia terminologies. So it means that we follow their suggestion that only plainer sheet like tissues can be called Fascia.
That means he a killer standard and is no longer a fashional tissue for this anatomical definition. So it needs to be sheep lie and it needs to be so dense that you can cut it with a scalpel. So you can make two pieces out of one piece. So that means in this more specific anatomical definition that the tendance, uh, and the aponeurosis are not included because they are so specialized connective tissues. Also the Endo Museum, which is a very, very tiny tissue around a single muscle fibro is no longer included because it's too small to split it. We are with a scalpel. So so far we are in line with the medical anatomists and when you're speaking with them we suggest to follow that terminology and only call Fascia those tissues that you can dissect with a scalpel in a clear way and that are in a sheep like uh, arrangement. But there was also a decision and we suggested to call that usage a Fascia.
So the Achilles standard is not a Fascia, which is very specific, but, and this was the second and also a very important decision and maybe more relevant for you when you're looking at movement orchestration. When you're looking at false transmission, for example, in stretching. And when you're looking at sensory capacities like nosy ception, where is the pain coming from? The back pain for example, or the neck pain and most important propioception. Uh, so when you look at proprioception, where do people feel their body? Which tissues tell them about the movement. Then we are talking about the fashion system and then the achilla standard is part of the federal system because we come off from a functional perspective.
So far, the first terminology, we already had a clear agreement of this powerful meeting that has been happening there. The functional definition needs to be chiseled out more clearly, which tissues will be included and which one not. And there is now a new committee that will be working in the next year to come up with a clear definition of that. But there have been proposals in their direction and most likely the new functional definition of the federal system will be quite similar to what our group had proposed a few years ago in which all collagenous fibrous connective tissues are considered to be part of the fashion system or the body wide fashion network. So bones are not treasure. They are connective tissue Fascia only.
Those connective tissues which are primarily tensional, Li loaded, not compression only loaded, you need those. So connective tissue is a much broader aggregation of tissues and faculties use are those who are primarily stretch loaded. So that includes ligaments, joint capsules, a, the endomysium around single myofibrils, but also the [inaudible] museum that's covering a whole muscle. So it's a much wider terminology that we are using. And uh, this child here says it Clyde nicely. Each of these two terminologies has its advantages.
For example, if you are describing forced transmission, then the specific anatomical terminology is not so good because the force from your hamstrings goes all the way down in the Fascia covering your car's muscles. Then it gets into the aponeurosis, then in the Achilles Tendon, then into the heel pad and then into the Plantar Fascia, plantar ligament, plantar aponeurosis. All these names are out there for, for us, we don't care. It's a force that travels wherever you have college and fibers connecting tension all forth with each other. On the other side, if you're looking at tissue repair, proprioception and nociception, the functional definition is also much better, but when you are communicating with medical professionals who are used to a very specific lens and then you make life for them easier and for yourself easier. If you distinguish between maybe proper fresher and connective tissue in general and then you can acknowledge well for you, proper Fascia is only sheet like connective tissue. Now let me include the aponeurosis. Let me include China capsules, et Cetera.
For us it means when you're talking with embodiment oriented practitioners and with clients, then the functional definition of the functional of the federal system makes a lot of uh, or has actually the more advantages. So so far so good. So you can continue to use Fascia for a lot of things, but you should know that there is also a more restrictive and you can say, okay now we use your anatomical definition and we also have a functional terminology that is not so unusual because for example, if you talk to a botanist that a fish, a dolphin is not a fish. So there is a general language and there is a specific language, but for many people that also is a fish available as a fish. So you have specific languages. Also,
Chapter 3
Three Layers of Lumbar Fascia
what has happening just recently in the last few years that traditional concept have been re-examined about the false transmission and one of the most powerful and influential concepts about my official foster and submission is that of my Robyn colleague, Thomas Myers, the so called anatomy trains, very powerful concept, very useful.
I highly recommend his book and I highly recommend inclusion of that concept into a pill artist practice, but also into yoga practice, et cetera. Now, young Wilker from the University of Frankfurt has done cadaver studies to examine which of these myofascial, uh, anatomy trains has a high anatomical evidence. So if you pull here, how many millimeters does it spread towards the left shoulder and towards your right shoulder. So you can actually do quantified studies about that. And based on that, basically the maturity of the anatomy trains has very good anatomical evidence there because to make nice drawings is convincing. It's also possible to draw something out of a cadaver.
But anybody who has done dissection causes, you know that you can carve almost anything out. So if I give you a piece of tree, you can carve a naked woman out and say she was there before you, but somebody who else could carve something else out. So the demonstration that Hamas has been doing in the past, they were convincing for lay people, but they were not yet convincing to the critical anatomical scientists. Now, thanks to Yan Willka and this new publication here, the maturity of Tom Myers Anatomy trains are now convincing two critical anatomical scientists, particularly the superficial back line that we will look at. That goes all the way from the new kill ligament, erectile Spina, all the way down to the cops and even to the Plantar Fascia down there.
Also the functional back line that crosses from the Latissimus Dorsi and it's upper neurosis to the contralateral gluteus maximus and going down on the opposite side. There is a lot of evidence for that. Many studies have shown that an f quantified that and also the functional front line. Also, the superficial front line on the other side has very little anatomical concept. It was a nice concept, but it's probably not very convincing if you do quantified studies on it. On the other side you have moderate evidence, so at least in two or three transitions of the many transitions described, it has been found to be congruent with anatomical research regarding the spiral line and the lateral line. So that is good news and it's a, it's useful for you. So when you use these lines, I will apply it now to the latest insights about low back stability. And after my lecture, my wife Will Miller.
We'll do a practical workshop on how to work [inaudible] three layers of lumbar Fascia for a healthy lower back based on stretching, Pilatos Yoga and gymnastic movements. And she will specify which layer she's focusing here because that is new now. So rich fashionable layers, which my professional connections are responsible for which portion of lumber or low back stability. The first layer has been already included in Tamayo system and that is the layer that attaches to the spine as processes and where a lot of the fibers, but not all the fibers cross to the crown to control lateral side. So if you want to strengthen that layer, you should not only do trunk movement, but limb movement.
This is part of this is mostly limp muscles. So if you do healthy bag exercises, when you include on your end, you exclude the arms or you exclude the legs because you say, I want to focus on the bag. You're not acknowledging the big importance for lumber stability. Of this first lumbar Fascia layer. So that was already examined very much in detailed in quantified studies in the mid nineties by Andrew flaming and other, uh, Dutch scientists, anatomical scientists. If you peel this layer, I love this picture here because it shows how big this piece of Fascia is.
If you peel that layer off, then you come to another layer that is also attached to the spinus process. And that is the superficial back line that Hamas has been focusing on. And there is a lot of evidence on that, particularly for the transition of a lot of fibers of the biceps Femoris, very important hamstring muscle I learned in school and for the exam that the origin of that muscle is at the issue of tuberosity at the sit bone that was good enough to pass the exam. But in order to understand movement, that is not good enough. It's not sufficient because a significant degree of the fibers does not attach at the sit bone tuberosity. It says, hello, is it one to Ross city I will not attach to you? I go directly onwards towards the sacrum and unites with the sacred tuberous ligament. And that also continues all the way up, mostly on the ipsilateral side as a facial envelope of the erector spinae muscle all the way up to the new Kale Fascia that you have up there.
So if you want to work with that layer, then you would do exercises with a straight leg and you would do not so much rotation, you would be going forward similar like in the slum position. So here you are stretching, you're loading the second layer of of the lumber fascia and if you don't do that for a couple of months, the second layer will start to lose its architecture to deteriorate. If you want to use a first layer, this would be the best position, squatting, but also reaching upwards and bending forward. So doing a roll on the floor, squatting once a while. All these are very, very, or doing prey or positions in a rabbit position, etc. That will be perfect for the first layer. But doing this, spending forward that you have a lot in [inaudible] in yoga is very good.
For the second plank and similar like if you own a tent or parachute, you need to open these layers once every month at least. Otherwise they will blue together. But opening one layer is not sufficient. So it's similar like you have different shirts on top of each other and you need to stretch each shirt also separately. Otherwise they are starting to glue together. So these are the two layers.
Both of them have been known already in the 90s so for anatomical scientists this is not so new. What is new is now very exciting. Also coming from Andree flaming and being reasonably published in the journal of Anatomy is the third layer of the lumber fresher that attaches to the side processes to the transverse processes. So this is a lumbar vertebra or half of number of Algebra. This is the spinus process taking backwards. These are the erector Spina, the back muscles, and this is a transverse process and this is a lateral belly wall and very interesting.
There is a very sick layer of Fascia in front of the erectile spina attaching to the trans process and this layer is twice as thick as beaus of the blankets that we just described that are attaching at the spinus process. So most likely for lumbar stability it is as at least as important as the two layers before. So if you goal is to be able to have your daughter right on your shoulder and you are stable enough to give her a good ride while while you're walking on the beach or to carry a big sack of potatoes on your back or whatever, if that's your goal and it is my goal that I have a bag that is healthy to give children that choice, then just having these two layers in a resilient condition is not sufficient. Most likely. We also need to understand and know how to load, how to train the resilience of this third layer. Now this third layer for understandable reasons, not so much has been known about it because you need long needles to get to the hair and I would have doubts to be a victim for that kind of research.
Also with the EMG, with electrical measurements, it is very hard to get there but now it's with new measurement methods. They have been getting more insights on them. Now this will speak to you as [inaudible] as instructors because this third layer there is one muscle that is influencing that the most and that is the trends. Whereas abdominis that is if I would ask you which joined is a transverse abdominis flexing or extending, you would have, well, it doesn't have a choice. Most muscles are very clear. They flex the elbow joint or shoulder joint, but the transverse abdominis is not a regular muscle in terms of moving a joint from here to there.
It is basically a fashion membrane Tony fire or titan or rep tension regulator and in in first order for this third layer that is in a value pardoned layer and the most important muscle to regulate that layer is the transparency of dominance and as you know from your research also from the very impressive research from Paul Hodges and Caroline Richardson from the Australian pds a, it is very common that this muscle goes into this function. Whenever you have low back pain, this muscle, the red muscle fibers say, I don't want to work anymore, let the other muscles take care of that. I'm not taking part in that club anymore. That not only happens in low back pain but also when you are under psychological stress or when you expect low back pain. Then with very good PLR, this training you can learn to activate that muscle again, but that muscle needs this fashion membrane to be in a loadable position.
If it doesn't slide, if it's glued together, then the red muscle fibers can pull as much as they want, but it will not transmit to the lumbar spine. So doing [inaudible] is only for the red fiber muscle fibers is not sufficient unless the right collagenous fibers are able to transmit the falls. If I'm pulling here and it doesn't go why or the Fascia to where you want to have it, I can exercise my arm all the way. You need to unglue the Fascia and then the transverse abdominis can exert its lumbar stability function on the, on the lumbar spine. So this is now a very nice model. So we have these two layers.
It helps him do the spinus process. The first layer would be involved in a squat position and contralateral rotation. The second layer would be here in the, um, how do the Australians call it? I used the name before slumped position. This is called, yeah. And the third one would be your core stability exercises as Steve or Mueller will show later in the practical session where you can do plank positions, specific sounds et Cetera, in order to activate the transfer as abdominis.
What is important for anatomies is there is a newly rediscovered triangle where the tension of the transverse abdominis goes either only to the transverse process. Why or the third layer or where this sliding switch can determine whether a portion of the tension also goes to the spinus process. So if you expect a heavy load, if I throw a very heavy ball towards you and you ready to catch it, then your brain, if it's intelligent, decides to call activate not only the cost ability, muscle of the transverse abdominous but to call activate also the erector spinner and then this triangle, if it is healthy, if it's not glued, if it's not stuck, we'll shift it a little bit such that the enormous tension of there catching the ball movement will transmit halfway to the spine is process and halfway to the transverse process. And then of course you are twice as strong so you can catch something without having an ouch micro injury and some collagen fibers in your lower back. So this is a very nice model.
So for the lower back you can see it like the parachute piece of cloth that they are using when different people are jumping out of the window. If somebody very light jumps out of the window, and if I throw you something by light, you may only need one or two of these fire man that are standing there. So you can catch it with your Latisse plumbers and with the Gluteus maximus only. But if I throw you a very heavy medicine ball, which is great lower stability exercises, if you do that in a prepared and modified manner, then all the sixth fire man should say we are ready. And then you maybe bending your knees, you may be doing a squatting, you're reaching out, and then you have a healthy fascia involved into that.
So this is a very nice concept about lumbar stability and the three layers of the lumbar fascia involved. Let's go on because now Helen large server has shown that the first and second
Chapter 4
Fascial Therapy
layer are prone to adhesions, particularly in low back pain patients in chronic low back pain patients. So this is ultrasound and ultrasound is now upcoming technology. Actually it gets into a price range. You can now get a decent ultrasound equipment for your PT practice for European artist practice around 2002 and a half thousand dollars.
That is good enough for superficial muscles, not for this so was but where you can see this is the skin, this is subcutaneous connective tissue that you can do a little fold with and here is the first layer of dense fascia outside posterior to the erector spina and first it looked like in low back pain people that this layer is thicker and now she showed it's only in man, it's significantly thicker when they have low back pain in women. There is an interesting group where it's sometimes get less sick and we don't know what the reason is for that, but in both groups, men and women, when they have chronic low back pain, this layer is more adherent. You could say because it doesn't slide so freely in forward pending. So if I'm bending forward and my shirt is free, it is free to slide half an inch in relationship to my muscles on the knees. But if I'm sweaty or if I have a gluing here, I may not be able to reach so far forward because my shirt is tucked together with my underwear underneath my skin underneath and that is happening in your low back pain patients.
So we don't know what the reason is whether that's cause or effect, but it is a factor to include in your treatment that you can assume if they have chronic low back pain at least for three months, for example, that the lumber fashion most likely is not able to slide and that restricts their movement. But it will also inhibit the appropriate section. If you ask a client with low back pain, do you have a low doses? Now do you have a round back? They simply don't know they need to use a mirror because proprioception comes. A lot of it comes from the sliding movement.
But if the sliding movement is restricted, they have little information, they'll come to join our club where we are right in the middle of it. So this is important that this layer of Fascia can glue together with the, with the underlying musculature. And then we are looking for treatment methods. How can we lose five Roddick tissue that is glued together in areas where it should be free to move. And then we come to stretching. We come to different self-treatment methods. This is a very dynamic field of exploration. Uh, this the same ultrasound they have also now looked at other muscles.
And this you can also do with cheap ultrasound where you look at the scalene muscles, all the sternal Clyde or muscles up here. And you look how thick this is. A muscle. This is again the subcutaneous connective tissue and the skin is up here and you see in healthy people on the left, the AP museum, which is kind of the sausage envelope around the muscle. So it's a muscular, the festal envelope rounded is only like a millimeter thin in people who have chronic back and neck pain. Not In all of them, but in many of them, if you touch it, it feels quite hard. Not because the red meat on the inside is stiffer, but because the envelope has doubled or more than doubled in its sickness, and this is very helpful now so you can use a ultrasound, but if you don't have ultrasound you can use your hand and try to feel is it the envelope that is sick or is it the sausage? The content on the middle that has increased.
If it's the envelope that sick, it's an unyielding quality on the surface of the, of the, of the structure that you're palpating and that will be very helpful. For example, I've been part of surgery with spastic children that is now developed in Germany. It originally came from Russia. We are spastic people who cannot get their yield down, mostly the cerebral palsy children and you cannot split their leg and everything has tightened. They do ultrasound before and in many of them their epimysium is two three millimeters sick. This is one millimeter. This is like three millimeters thick here and then they do a very minimal invasive puncture research, little round scalpel to make holes here and suddenly you can open the leg.
So they do it with local anesthesia. You are here and it's very impressive. The most impressive thing was for me the sound when this round scaple goes under the superficial Fascia, just like in piercing, so you only go like three millimeter thing and when he scrapes the Fascia it's a sound like wood or like a dry egg on the outside. I will never forget that. And then he scrapes the actual and the muscle softens. So it was not a muscular contraction.
It was an actual like thickening of the fashion envelope in these people. That was very impressive for me. Yeah, so the question is, is the treatment lasts by interesting. If they have good physical therapy, it lasts, then they don't need to come back. So I'm particularly talking about Dr [inaudible] is, he's one of the surgeons who are most pioneered in this [inaudible] method or pell Putaine, Myo, Palka, Diane Powell, Putaine Myo Fascia to me is a proper medical name for it. But if they don't have good physical therapy at least twice a week where they do end range fashion loading, then he sees most of them again a year later because the Fascia has tightened up again. So after the surgery they put these children into costs in end range positions and the surgeon does it himself to be, I give them these cars or only for few days and a few weeks there are so that they have minimal movement but that they use their body in long stretch position and that they get accustomed to it and then they need to do pee Lattus in yoga stretches and then he doesn't need to see them again.
So if I can rephrase part of the question, rather there is a mind body connection that you can see in the fractional thickening and also in the functional effects in these children after the surgery. The connection that I mentioned about people being afraid of low back pain. So if you come with a needle and say this is gonna hurt a, that connection has only been done to the erector spinae muscles and to the transfers of dominance not as the first year. So that research that I was referring on that is pretty solid, but it's any works in seconds and you can measure in EMG. Fastenal sickening usually does not occur in seconds.
It occurs in weeks. So fascia is a much slow organ. So that is important. But we have been exploring that at own university rather is the slow speed that Fascia has to adapt to different stimulations. Does it adapt also to chronic stress? And that was an old question. So we tested faculties use in response to Adrenalin, Acetyl Colin neurodrive, Anil into these uh, autonomic nervous system transmitter substances.
And we were first frustrated because we couldn't find any connection. Fascia does tighten, it does relax, but more in relationship to biochemical substances that are related with inflammation and with wound repair. But then later we found a connection in the literature that there is a connection from chronic sympathetic charge towards a specific site akin that is called TGF transforming growth factor. And so if you are under chronic stress, your body produces more of the teachy f and that. So it's an indirect connection that is the most potent contracting, stimulating substance to get facial tissues to become tighter.
So there you have an indirect connection. It's not done in split seconds. Why are neural soon lapses? So it's more done in a background, slow side token way that is not so specific but more general. But that explains that when people have several months of very stressful periods in their life and it does happen, you know you have an exam, your children, your divorce, everything and you have mopping at your job and you see these patients, you have seen them once a week in the years before and then during the stressful period you touch them and it feels like their Fascia has gotten thicker and as if they have gotten eggshells under there. So there is no study that has shown that yet that people, when they are under stress that they have figure Epi Museum. We only know that from people who have chronic neck pain.
Not all of them, but the majority has that and we know it from these spastic children. But that would be very interesting too to be able to evaluate. So either you can use ultrasound in the future or you can use your hands to a, would it be one of these eggshells that Robert described where if you were able to have the muscle under your hand that it would be almost dry and very, very thick. And then the question is how can we, if we are not surgeons, uh, so, so how can we tell the cells, the fibroblasts that produce Collagen, please don't put you so much collagen and make this actual a little bit, you know, in the future. And that's where you work comes in. So this is quite quite exciting because you can also in the future differentiate when somebody has a replenish injury and they have chronic neck pain for months, sometimes for a year, years afterwards. Rather they can profit from Fastenal syrupy or not, not everybody profits from functional therapy.
And one difference can be is a hardness. If there is hardness involved, does it come from the sausage content from the red acting myocin muscle fibers or from the whitish x shell envelope from the outside. So if it's the envelope, then of course a good fasher therapist is, it's very helpful. So this is based on very, very good pioneering work from the stakeholder group in Italy. I highly recommend their writings, but also the manipulation therapy that they have developed in the last couple of years. The biggest, the two big names is color stucco and Antonio Stucco and they have done a lot of these pioneer young studies mentioned there. Now if you look at the different components of Fascia,
Chapter 5
Components of Fascia
we have looked so far at the fibers, but Fascia is con is composed of much more. And in terms of terminology, let me briefly clarify that because I will use it later on.
Specialties use like other connective tissues is composed of cells and of non cellular material. Very simple. And the specifically of connective tissue, particularly especially connective tissue, is that the cells make up a minority of the volume only. This is very different as muscle tissue with neural tissue covers liver, liver tissue. So connective tissue is similar like an end pile where you see all the stuff that the cells have built together. But you may on your first site see no and their, because they're hidden inside.
So the building that the cells have created is a hundred times larger than the architects himself. So this would be similar to somebody looking at Manhattan at night. They see all these strange buildings and streets and skyscrapers, but they don't see the living architects and my advises, if you want to change the city, talk to the architects. This is a much more long lasting sustaining therapeutic approach rather than you tearing the college and fibers into one direction or the other. So this is important. We have mostly, most of the cells are connective tissue cells that are now called fibroblasts.
Nobody uses anymore so much as it was done 10 years ago. The distinction between fibro sites and fibroblasts, we call all these connective tissue cells that are able to produce Collagen, but also to produce a big part of the ground substance. We call them fiberglass and that's a maturity of themselves. So then what about the 90 something percent of the volume that is not cells? This is called the extracellular matrix and that is composed of fibers and out of a liquid gluey ground substance and ground substance and extra cellular matrix is not the same. That is often confused in other writings.
So extra cellular matrix includes the fibers and includes a ground substance. And now when you look at a federal gluing, a federal thickening, the question is does the stiffness come from the cells, does it come from the fibers and or does it come from the liquid ground substance? And then you have different therapeutic avenues and strategies to follow to look at them. So that is quite helpful when we now look at what happens in aging and here you see the Collagen fibers in a six year old as opposed to the more crisp and brutal and chaotic and more fresh our culture and fibers in a 90 year old. And that is a development that you can slow down but you cannot completely reverse it or halted.
So when you will be 95 years old and your lumber Fascia is being stretched and you do the same movement, part of the different why you don't have this elastic recoil anymore is because the architecture of the Collagen fibers has changed due to aging. Uh, this is also happening not due to but also due to immobility. So when you have a cost around your knee joint for several weeks, then the architecture of the college in fiber that used to be more regular. For example here, it has two main directions. The one direction that I am pointing on from Lebron from left up to write down, but it also has the second main direction.
Whereas if you are not applying movement for a long time, then you get a key arctic proliferation of Collagen and then it is more like a celt tissue that doesn't have an elastic quality because the fibers just like in Feld going all different directions so your stretchability, your resilience will not be so good if you have this fibrosis proliferation and that is happening in people who are couch potatoes, they have the hip joint which they never use in the end range position or in the stretch position or in this position and then the fibers who are able to accompany in this position, they are starting to glue together in a felt like fiberoptic condition and when you then want to go in that position you realize, oh I'm getting old there but it may be just your couch potato in mobility and not using the blanket and the parachute in the angles in which it was designed to be yours. So that is related to the fibers in there and there fiber grows. Very interesting is very much influenced by gross hormone production in the body. And that is a more and more coming as a question. I'm sure you will have questions at the end when we open the question and the answer part. What about nutrition, what about water drinking, what about supplements, et Cetera. And there is a lot of dynamic new research happening.
Nutrition for healthy connective tissue. Not Everybody wants to have big muscles, but almost everybody wants to have healthy connective tissue is in there. And the most potent hormone for that is the human growth hormone. And we know that is declining as we age. And Eh, there have been studies in Human Growth Home on doping or supplementation and there have been big hopes to it and a lot of big benefits have been shown, but also negative side effects.
So most people don't advise to do doping with human growth hormone. Fortunately it did not show muscle growth, otherwise millions of people would be using that who want mostly men like me who want to have bigger muscles, but to far reasons that are not completely understood. The muscle cells do not respond to to the growth hormone bones response ligament response. Almost every other tissue does respond. So it's no longer used for doping or not used as much in doping, illegal doping in the bodybuilding scene. They'd take almost any other drug on this planet, but this is not so much used anymore because it doesn't build up muscles, but it builds up a bigger, stronger connective tissue.
Now, if you don't want to do doping, which I don't recommend because it does have side effects, then you can learn what are natural enhancers of human growth hormone. And a big one is sleep. And maybe the reason why all people have less growth hormone is because they also sleep less and it's produced in the non-rem sleep. So not while you're dreaming. So in the dreamless periods of the night, but in the later portion of the night. So in the first one or two hours, you're not producing much growth hormone, but after four or five hours, so in the last cycles of non-rem sleep, they are, you have the growth hormone produce. Guess what?
This is what's lacking. As we get older in many of us, and that may positively explain why our connective tissue gets brittle in that. So it would mean if you want to do something for your connective tissue. Also look at your sleep habits, whether you once a while have sufficient sleep that has these advanced stages of non rem sleep phases included there. If you're live for many weeks without sufficient sleep, maybe your memory is functioning, your muscles may be functioning, maybe your cash inflow is functioning, but you're a careless tendon, your lumbar Fascia, uh, the scalene envelope, uh, you know, kill Fasher will become more brittle. It doesn't have the juices of the human growth hormone that that is like a fertilizer for the architects, for the cells. So this is very interesting.
The second, uh, most important enhancer for growth hormone is challenging exercise and I didn't like to hear that, but it needs to be exercise that gets you into an acidic state. Then the body says, I have had too much. Now I need to do something against it. So if you only exercise only according to your comfort zone, this is ideal for many things in your body, but it doesn't pump up your human growth hormone. I'm not recommending to do that every day. So that will, because you also need the appropriate challenging stimulation of exercise.
So think sprinting, not modest jogging or weight lifting, but it needs to be exercise where you feel exhausted or partially exhausted afterwards and where you feel like it's good to have a rest for one day or two. So this would be healthy not to have every day but maybe once a week or maybe once a months because that is doing the same as long nights of sleep. Guess what? People with Fibromyalgia, they have neither. They cannot sleep much because of the pain they have and they don't exercise because whenever they do exercise, they are punished for it. They have more pain afterwards and before they should exercise.
But who is doing exercise where when you feel worse before people with low back pain, you do exercise and you've and you curse before. But after that you say that was good. You know, you should kick me in my eyes afterwards. But people with Fibromyalgia, if you are their coach, you say please do exercise, but they kicked you twice in the ass afterwards. So it's no fun for the coach. It's no fun for them. But they still should be doing exercise. But of course they don't for understandable reasons. So they lack these tools. Very important suppliers, enhancers of Gross Oman.
And that is like, you have a lot of architects but they don't have building material. You know, they are drinking too much alcohol. So what CD, well, what n pile, what Manhattan skyscraper buildings, what college and fibers can you expect from, from them. And then also regarding nutrition. Basically high insulin is an antidote for human growth hormone. So if you have an eddy post person, if you have a pre diabetes vedic person that is lowering the or if you eat a lot of sugar or high glycemic drinks for example that is bad for many things but particularly bad for your connective tissue because then you don't have so they recommend if you want to uh, guide your nutrition in relationship to connective tissue then a more high protein diet is more beneficial because it includes all the amino acids that you use for human growth hormone and later also for college and production and this is what I got out of the literature. It's there is a so-called CDP Collin that seems to be number one out of these amino acids.
Then Guinean and [inaudible] they are already known because they are good for the blood vessels and for nitric oxide production which is her and very important a transmitter in our body but also glycine, glutamine and this vitamin B three they are important. A shortcut has been developed by key spa and there is a very nice article in men's fitness, which I would have not expected on nutrition and connective tissue based on the research, partially of keys bar at the University of UC Davis in California. And he has also looked at which ingredients should nutrition have for bodybuilders and high for high performance athletes that they have strong tendons, strong ligaments, and resilient Fascia. And he came out with a solution where he said, it's basically gelatin. Gelatin is made out of Collagen from animals and it has already all the ingredients in it. So when you try to give cello to bodybuilders, they didn't like it because they don't associate that with, with muscular strengths.
So now he sells it for a lot of money as powder and they love to take that. So if you want to eat cello at home because you're not a bodybuilder, it may be a beneficial mixture of different amino acid for healthy connective tissue. So if you do a a phase in your life where you say, I'm investing, I have my yoga teacher exam and two months in I want to be very good there so I want to rock with my connective tissue where all you have a wound and you have low back pain that's associated to the Lumbar Fascia. How can I tell my cells to heal that very fast? I would eat cello twice a week maybe based on that, but you can also take all the different supplements individually. So this is quite interesting when looking at the fibers.
So a lot of Collagen pathologies, fatter pathologies are based on the fibers being too thick or being glued to uh, to each other. Now the Staikos have proposed that we should differentiate between fibrosis. This is what I've shown before in which the actual has grown and become too sick. So you have an additional growth of Collagen fibers in there and that could be due to overload. It could be also due to immobility they are in. We'll look at that later.
But there is also an interesting condition where you don't have increased college and fibers, but in which the Louie substance goes into a more sticky condition and that is often related to higher Llorona as a proteoglycan that is sometimes slippery, but it can also become bluelike and they showed that here for example, in some people you have two layers of Fascia and you have a thick layer of glue in between and then you should not look so much at Collagen, but at the ground substance, what kind of Hyaluronan do I have in here? How can I influence that? And the new research from Antonio Stecko and Tom Findlay, not yet ultimately soundproof. It's not rocket proof yet, but it indicates that within one or two minutes of applying rolfing like pressure, you may change a glue like Hyaluronan paste into a liquid slippery. A film where our federal envelopes can slide on each other. If you, if you can do that with an ultrasound head where you put five kilograms of pressure, 10 pounds on it and you see this is happening, that's what they are reporting to us. Then you can also do it on a foam roller for example. So this is quite a quite interesting that we may have some stiffening, uh, some lack of mobility in your body.
That's not because the actual being too thick, but because of too much glue in the proteoglycan rich round substance in the connective tissue in there. Now how can we influence the ground substance? Two thirds of the ground substance consists of water and a very plausible approach has been then we just need to drink enough water in order to prevent our ground substance from getting more dry and more glue, like very plausible thinking. But apparently this is not so easy because the water in the ground substance almost never gets there by more supply and by pushing down more water in the outer y'alls, all the water in there is pulled in by suction and that is limited by the collagen fibers and by the cells here. Basically all the green material here is thirsty for more water but it cannot get more water because the pockets are held tight. So there is a lot of higher Ronan in here and it wants to to drink at least a hundred times more water than it already has.
But if I would drink more water, if you or drink more water, then we would need to separate more than we allow to. So the college in fibers prevent us from drinking more in today's always thirsty proteoglycans in there. When you have injury of when you have inflammation, then you lose in the college and fibers here and then I can suck in all the water I want no matter where I get it from. It may be from your pizza, it may be from the bread your, you don't need to drink the water, you need to make the ground substance thirsty and this is a picture that fits to it. If you float more water down the river, it may not help the starving land at the site. You need to create Osmotics suction in there and unless you have that, you can flow down the best crystal water of this. Well down there, it will go out your sweat glands, but it will not get into your plantar Fascia. You will not get into your Keller standard or your lumber Fascia.
So doing things can still be good, but it's not the solution to influence the slippery nose of the ground substance apart from some very rare conditions. So there are some diseases or they're very old people, they are sense of thirsty, often isn't at war, but the people that come to your studio that are below 90 drinking more does not help them, at least not with their connective tissue. Too Bad. It would have been an easy solution to get in there.
Chapter 6
Davis' Law
So now we have looked at the different pathologies happening and now are come to the Davis law, which is basically a specification of so-called devolve slaw off Slava is two f. Some of y'all remember that from longtime ago.
It describes how bony TCU is able to adapt its architecture to challenging loading. And you may have seen pictures of the trabecular of this very intricate architecture inside the bone where you see on the side of the bone where you have most loading there, you have a lot of the pockets there. So it means this adequate loading connective tissue, particularly bone and connective tissue can adapt to the loading such that it's better equipped to, to resist the same loading. And that has been shown in many ways. It's a big problem with astronauts because they don't have sufficient bloating.
They're doing all kinds of vibratory machines but that's not completely preventing their aging process. So they are getting osteoporotic when they are in age and they can recover some of it but not all of it. So it means you need mechanical loading in the appropriate manner for the architecture of the connective tissue to adapt to that. And this is a very nice drawing now because it has been now applied, uh, to fibrous connective tissue of his bones. It had been known you need about 1.5% defamation, which is a lot for your FEMA before you are asked to anti osteoporotic program.
Has any effect. So bouncing is good for your limbs, it's good for your brain, but it will not make your femur less osteoporotic. If you do that, you need like two or three times the body weight because then you do have this one and half percent defamation where then the osteoblasts say, Oh holy couch, my heart is too shaky. I need to strengthen some of the connections on the inside. So that is pretty much known in Osteology, this Amar specific application. You've also find that in Wikipedia is now a more recent topic of research because you see the same thing. You have the danger of overloading where you land, you lose the integrity of the connective issue and you have underloading there and we'll look at that in a minute more specifically.
Then you have a wide area where you don't get better and you don't get worse. And that is a question for some of them. You know, how little artists do I need to do in order not to lose everything, you know, is once a month sufficient? Is is once a week sufficient? Uh, the answer is of course it depends. If you are high performance athletes and you want to keep your level, then practicing it once a month will not keep you at that high level. But if you are a mediocre person and you have never been very strong, never been flexible, but you say in the next half a year, my kids sign a priority. My house needs to be built.
I want to cut down on my body program and in two years I will have all, you know, I will live in Santa Barbara, I have the beach in front, but before there I need to make money or whatever. Then the question is how, how little can you practice? So if you have a mediocre level, it may be every two weeks, every one week, but not every three months. So if you never do a roll forward or a squat position or a stretch for three months, you will lose it gradually. But if you do it once a week and you have been not a high performance athlete, it may be sufficient for that gray zone of loading. You don't get better, you don't get worse. But there is a lot of variation in it.
And now the interesting thing comes there is a small green Arrow and unfortunately it is a very narrow pass only where the tissue get stronger and more resilient and adapt its architecture to be better equipped. And that is just very under the overloading phase. If you do less, nothing happens in there. And that is now the question, how strong do you need to load the Achilla standard that it improves its, its architecture and its resilience? And the answer is it's probably around four to 5% for tenants and maybe two or 3% for intramuscular connective tissue. And we'll need to look at that.
How much that is. Let me blow that chart up to make it more specific. Basically here you see this is healthy tissue and that the fibrotic tissue that you get actually in both of the red arrows there. So let's start with uh, insufficient challenge that is a couch potato or somebody who is immobilized, who has to lie in bed. For example, a where's a cast, which is terrible because then the connective tissue starts losing its architecture and that's what you see here. They develop a fibrosis that we have seen there.
So you lose the regular architecture. You don't have letters like criss-cross, a two directional fresher that you often have in other pieces of the body. You have multi directional arrangement. Uh, very interesting there Perry museum, which is a envelopes around muscle fiber bundles, not around, it's not the actual on the outside it's more partial eggshells on the inside of a muscle that gets sicker with, with immobility. And that is quite interesting because we are, we found there is a lot of myofibroblasts. These are fibroblasts that are specialized on a title contracture so that may be related to them.
And interesting area for nutrition are the age like age advanced glycation end products and that used to be only familiar with people in diabetes. And now everybody who is interested in aging less rapidly should know about age. These are large crystals that are formed out of carbohydrates, for example, out of complex molecules. And you ha and that makes it more crisp. Everybody who is a good baker and a good cook knows about the so-called may lot a reaction where you make a piece of meat more crisp or call som or crisp where you heat it rapidly in such a way that the same material forms large crystal and that tastes good to our tongue. Now guess what? As you get older, the more crisp your Achilles tendon gets. If somebody would eat you, they would say, oh, very nice.
90 year old homosapiens very crisp, but I don't want to be eating it. I don't want to be crisp. I want to be a lastic and resilient, so I don't want these large crystals forming as rapidly as a we'll be doing when I'm a couch potato. A good picture is if you have a glass of honey and you keep that immobilized for a long time, it will start forming these crystals usually on the outside. Then there is a reversible period. If you then come and steroid around, these crystals can be broken up, but if you come too late, the crystals will not break up and you can stay around forever.
And that's exactly also happening in humans. In prediabetes there is a period of about one and a half years. If you then do exercise, you can loosen up the crystals. If you do it too late, you only starting around two crystals. So there is a lot of research we are related to that and they now have measurement methods where you can look at the skin and see how much crystals sphere you have in there. And these are not good crystals. They, they are bad crystals that you have there and they are mostly formed by bad nutrition but also by lack of stirring around.
So please stir your body around every piece of it because if it's, if it's stagnant, it will form these crystals and then you are have a crisp, a killer standard. I don't want that. I want it to be slippery to be moving and this is very important. So that's part of the underloading that you have there. Of course, then you lose stability and you lose. It becomes hard. But similar, like a biscuit basically is stiff but it's not strong. So similar, this also happens, we have is aging.
It becomes inelastic if you want to lengthen. It increases its resistance very rapidly, but it also breaks sooner. So the ultimate breaking strengths deteriorates. And that's where when you are a couch potato and you chunk down from a little stare, uh, one foot to the ground, your Achilles tendon says pink, ouch. And gives in because it tastes and it looks like a bit squid. So you don't want to. So this is a red Arrow for underloading.
Uh, let's look at the Arrow for overloading. This happens when you have 20,000 repetitions per week of the same movement or up to 40,000. If you have less than that, then you're not so prone here. So this is a repetitive strain injury in the typist who is doing keep up movement or the thumb on the iPhone has over 20,000 hits per week. Then not everybody, but then you come in the dangerous zone. Not for this red Arrow, but for this red arrow.
And basically they both result in fibrosis. But the fibrosis here is a vet fibrosis, which is a veteran. So it's, it's watery, it has edema and inflammation involved in it. And that's where, so if you have somebody who loves to go jogging on the beach, if they do that five to seven times a week for 20 minutes each, already they have an increased likelihood, not for that Red Arrow, but for this arrow. If they only do it three times, four times a week, they will have less likelihood of this red inflammatory overloading that many joggers have. So there is a repetition threshold. So people who love sports, they need to know about the overloading and that goes along with inflammatory cytokines that we have there. And then you need to know what kind of nutrition, what kind of rest, what kind of stretching is a good anti inflammatory medicine that you can do.
The new research from Helen logical but also from Paul Stanley has shown that a long duration, five minutes long stretches, particularly at a small magnitude, can have a very beneficial effect for inflammatory wound healing phases. So the wound heals faster and you have an enter time. So you can do a stretching not to become more mobile, but in order for your inflammatory pathology to heal back faster. So if you have somebody who has been jogging to such an extent that they get the runner's knee or that they get plantar fasciitis that's now called of our shows is there and you and you think there is a inflammation or swelling or heating involved, which is not always the case. Then doing five minutes long stretches at the beginning of the linear increase.
So, so you go with the finger until you realize going further will increase the resistance. And if you do that for five minutes, that will have an anti inflammatory effect on that. So this is this red era. And now this is what we are interested in here is what kind of conditioning is good to build up resilience in, in, in the federal architecture. And that is pretty similar to what is called super compensation in the bodybuilding, uh, sports athletic community. And it's actually quite similar.
You need to come with a moderately stimulating load to the fibroblasts, about 4% if it's in the tendon, but you don't need to repeat it very often. So maybe 20 jumps is enough, but it needs to be like two or three times your body weight. So you do rope skipping, 20 jumps, not 500 jumps that doesn't do more. And then you give it time to recover to that, which is usually one to three days depending on how old you are, how active your metabolism is, and also how strong has been the exercise loading on it. And if you repeat it, then you get an increase in strengths, increase in the Collagen will, new renewal rate.
So how rapidly does collagen regenerate itself and also in the elastic recall step air capacity. So if you want to become like an elastic springbok or like a kangaroo with your plantar Fascia, this is what you should exercise. So appropriate loading with sufficient regeneration time afterwards. So now let's see how the, so this is the Davis law. It's very interesting. Uh, it's, uh, basically it has shown that for intramuscular connective tissue, it may be sufficient to have half of your maximum rate on the Lumbar Fascia.
But for the tendance you need like 4% a longer duration, which you get with close to maximum loading, 70%, something like that. And that's different with special training as opposed to muscular training.
Chapter 7
Collagen Synthesis
Collagen centers is very interesting. Seems to happen faster than I have been telling those of you by year two years ago or in my lecture on fresh, the science principles. So I used to think that the half life of Collagen is around one year.
So it would mean after one year, only half of the college and fibers are uh, replaced. But now this new research says that the intramuscular connective tissue actually is much faster. So it has this oh 0.2% per hour. So it would mean already in half a year, most of the college done for fibers, those that are regenerative are already replaced in the tendons. It seems to be twice as slow, uh, because if you see here, it's only oh 0.4% power probably because tendon are more inert. That means the cells are not so active.
They are less cells in there and there is also less blood in them. So it depends how active your connective tissue is, how quickly it regenerate. But on the other side, they show that in the Akilla standard, which seems to be a very specialized ferarri human evolution development. Uh, there are a lot of fibers in there that never get replaced after you are 18, 19 year old, which is called skeletal maturity. So they looked at particles in the air but also in human body that are in the atmosphere of this planet. Since channel [inaudible] or since the very first nuclear bombings that have been done in the 60s and in my Achilles tendon, I was already 18 year.
I had already met a mature killer standard when channel [inaudible] happened. So most of my college and fiber bundles in the kill, kill 10 don't have these radio isotopic markings in there. So it means I kept the same fibers in there and that's not what I want to hear. But that seems to be the case. Maybe all the vulnerability of the Achilles tendon that is very, very specialized tissue. Uh, no other primate has such a long elastic cord that we have in there.
So it may be more prone for injury. So in general, yes, the human body adapts versus college and faster than we have resumed. So already in on average every seven months or every week, every year in attendance you have complete renewal. But not all the fibers get renewed in it. But in general, it's much, much slower, uh, to do federal training. And somebody says, I have three weeks time, I want to have a sexy body and three weeks for important reasons. Can you help me? Uh, it would be good to tell them, go somewhere else. Yeah. So, so go the toe, go to the muzzle term, go to the weight loss gym. But I cannot give you healthy Fascia in three weeks, but I can give you healthy Fascia in a matter of seven months, maybe even three months. So the, we have seen some studies that already between nine and 14 weeks show a different fashion architecture when it has been appropriately loaded according to Davis law. So you can, if you want to have a six pack that doesn't have more volume but more tension in the inscriptions in here that is then not based on muscle training but on fashional quantification, then you can get that hopefully in three months if you want to have that, their muscle grows, you can get more rapidly than you have that.
So now we know that connected to this, your response for loading, that it needs to be appropriate loading, but also what happens when it doesn't get appropriate loaded and also what, so what time frame you need in order to influence that. A big factor that we are now looking at. The third part of this lecture and where we have to develop these new mobility tests that I will then introduce is also your genetic constitution. And every yoga teacher, every pill artist teacher knows that they are people in the class. No matter what you do, they are quite stiff and they have been coming to your classes since months and you'll see small improvements, but they ask you, will I ever be able to be as flexible as the girl in the first role?
And if you are lying you say yes, please continue. There is hope for everybody, but you know, of course they will never be able to be so flexible as a girl in the first row. And that has not to do with their traumatic childhood or that they drink the wrong beer or anything like that. It may have to do in many cases with their genetic constitution. And that is important to understand.
So we have to develop this type ology that a, the connective tissue architecture is different, as different as a body shapes are or hail shapes are in, in people that there is a genetic variation there. On the one end of the spectrum, you have what we call the Viking body type who is genetically favored for eye high stiffness. So for them to carry their daughter or heavy load on their shoulders is easy because they will not have [inaudible] slipping out of place. So stability is very easy for them. They don't need to work hard to get that, but, uh, mobility is something that is lacking in them unless they really focus on work on them.
They are called Viking because they are prone for the so called Vikings disease, which also is called too between contracture or Palmer. Find fibromatosis that you see in men over 60 every fifth's hazard that they have a sickening, not of the muscles in the, in the hand, but of the palm of Fascia. And when they sleep, they fingers are curved, not because of the red muscle fibers being contracted, but because of this Viking's disease. Uh, that is quite popular in people whose ancestors come from Scandinavia. It's almost absent in people from Africa and from Asia except for one region in Japan where they immigrated from Scandinavia. So when you are proud for the vikings disease, then you are also more prone for scarring, so every half an injury, then the myofibroblasts are more active to make a sick scarring there. So you have a, the wound closes faster, which is an advantage in nonmedical clean conditions for survival.
But you also have big scarring afterwards. And the same people are prone for frozen shoulder mall more than others. And for a what's called mobile's letter hose, it's a vikings disease on the bottom of the foot. And there are several other fiber Arctic diseases. So if your ancestors have been coming from Scandinavia and you realize that you have a tendency for scarring and many people in your family have these nodules in the hand, then you may have a tendency towards a viking constitution.
Um, they are also more prone for ankylosing spondylitis. That is also called vector ef. That's much more common in men. And that's also, or a rigidity of the spine that they have there. And the theory from Alphonse Mazi and also under e flaming is that this may be an advantage in arctic conditions and Arctic conditions. Um, you need to create heat and the best source for heat is muscles and the more your muscles are glued to each other, the more friction they create, which each step that you're doing there.
And so you create more heat by the friction that you have. Although in Arctic climate it will be very easy for you to carry a, an injured child on your shoulder and a rain d on the other shoulder and to walk for two hours without needing to stop to get your lumber rider brought back in case or anything like that. So an IX body is good in an arctic climate. Cleopatra with her slipping disc, she would not be so well equipped, but put the Viking now in a tropic climate and it will be not so good or whether it's in the jungle for him to move from a to B and there is all kinds of trees and plants in between where he has to duck into swing over for a stiff over leaks. This is not very advantage also to run fast in the open Silvana is a much better to have a long, a killer standard that you have more in the other body type that I'm describing now. So this is an advantage for Arctic climate.
So if you have such a stiff where I can come in to who you are, [inaudible] classes, don't look at them in the way that I looked at them. What's wrong with you? You know what terrible a curse is happening, but more for which environment are you a hero and where do I need to take classes, vizio if I want to live and cope in that environment. And I don't know whether I need these classes in the future. So I better keep good relationships with you. Yeah.
But also why are you here? So stability is easy for you. You are here all, you are a real hero and uncertain. But if you want to tie your shoes on your own, maybe I can teach you something from my small long knowledge that I have. So this is important to know. It's not a pathology, it's a specification. And who knows what our future will be like.
Maybe they are the ones so they can sit in front of the computer maybe for nine hours and their neck is not hurting because x Sheryl is two millimeters sick. I am not there yet. I need to get up and move and somebody else does the work. So it may be an advantage for them. On the other side, you have what we call the bend new Wendy's or the temple dancers. Eh, I like the image of the temple dancers because the Indian temple dancers, they can hyper extend their fingers at least 90 degrees. So if I would do Indian temple dance here, it wouldn't be so beautiful, you know? So I could entertain you for two minutes but not for two hours. But there are Indian dancers, they can entertain you for the, so they are doing flowers and everything there.
So just for the entrance exam they need 90 degrees of finger extension. You would break my finger joints in order to get me there. So I'm more working there. And interestingly enough, these people are hyper flexible almost everywhere, not only at their fingers and they have not worked on their fingers. Many of them they have that from birth there and uh, they are also more prone for scoliosis. So you see that more in these flexible women.
You don't see it in round [inaudible] people who are out there that are looking like liar liken Obelix, they are more immunize obelisks body types who have no neck and round heads and are more in abduction, Eh, who are more Mesa [inaudible] they are immunised for scoliosis partially but they are more prone for ankylosing spondylitis, which is a rigidity of the spinal structure. So here the temple dancer is more prone for scoliosis and they are possibly better equipped for tropic climate. So they can go through the jungle but they also have long Achilles tendons so they can do this so they don't overheat when they hop through the savanna because they usually are elastic recoil that you have in there for and I'm going
Chapter 8
Hypermobile and Wiking Test
to use you if I can, uh, for the hypermobility or mobility, there is already a very nice test developed out there that are highly recommend. It's called debate and test for and that has been shown to have a high reliability. How you apply it. The different evaluators come to the same result but it also has a high validity in predicting. For example, if you have back pain and it's not really bad pain, but it's posterior pelvic pain, so where the dominant center of the pain is below the Iliac crest and you are a hyper mobile person with more than four points on this test, then you have a very high likelihood that more stretching there'll be not beneficial for you if you have posterior pelvic pain because then it's very likely that you have an increased flexibility around your sacral Iliac joint.
And then mobilizing Zac Hecho Iliac joint can get you short term out of the pain by distraction, but longterm it will be not helpful for. So doing this test can be actually quite helpful, but if you have more than four points, then you need to be more open to look. Maybe it's too short, maybe it's too loose, you don't know. So let me do this test with you and you can also do that yourself if you want, but are, but I will show it with you. So in this test, the first step test is you're standing next to me here. And just by using your weight, you're going down and you'll see whether or no problem.
So you see I would have to cheat with all kinds. So this will, I'm cheating. So the question is can you touch the ground with both flat hands, not just with one. So you get one point already four for their possible hypomobility. There is a maximum of nine points but if you get four then we say you are more on the Bendy Wendy's side and that will help us later on. So so what therapies you would be doing and what exercises would be good for you.
The second test is whether you can hyper extend your right elbow. Yeah, clearly. So you have two points and your left elbow also three points already. Yeah. So you can do that yourself. For me, I would have to do crucial torture to myself in order to compete with her. Not only with the forward pending tests.
So the forward pending only gets one point but you get one point for each side that you have there. Then you do the same thing with the leg. Whether you can hyper extend it now. I wouldn't say, I wouldn't say that. Yeah. So it should be a clear hyper extension. So at least 10 15 degrees of five high-brow extension. But you know how, how it looks like. So we are still [inaudible] three points for you there. And then we continue whether you can touch with the sump, your lower arm. No you can't. Yeah.
So you are as healthy as I am in relationship to that. But some of you can do that. Yeah. But, but you know people who are able to do that. Yeah. So you would get one point. Yeah. And you have not and probably you didn't work on that all your life. It's a genetic constitution that you have. So we are still the three points for you.
And there is a last test where you take the little finger and see if you can go 90 degrees and, and, and more. Okay. You can, so that's 90 degrees there. I'm not sure. Sure. Yeah. So you're, so we can discuss. So you have four points or four and a half you would say. Okay. So if you have somebody who has six points and more, then they are very, very clearly a person with general hypomobility that may be pain free. But if they have pain, then you have a via very high likelihood that mobile, more mobility will not be helpful for them.
But you need tonification and stability that the formula is teaching afterwards in the federal toning. So one test alone does not say anything. It's the sum of all of them. For example, if you have broken one hand and you don't get a point, it doesn't say anything about you to your genetic constitution, it says something about your life history. Yeah, so it's the sum of all of them. But this test has actually shown to be quite predictive to predict cases. Uh, there are two diseases where we are involved. One is called malfunction disease. The other is called a loss done loss.
They have so weak connective tissue that they are more prone for any reasons. So it means that blood vessels don't have the lst CT and you need to carefully watch them. And these people definitely need connective tissue strengthening, not connective tissue. Loosening. And we'll look at that in a in a minute. So this test is very much developed, but there hasn't been a test for the vikings. So we have now been developing in the last two years a viking test and I need to apologize.
It's not yet as crisp as a hyper mobile test is and it may never get there because as you Rosie, many additional factors are influencing that. But it's still good to see whether it applies to one person or to the other. Can I do that with you? Not that you are working, but you are probably more similar. Lie a lie. Like then I want to ride on shoulders. So, so you see how close can you get your hands behind your back? Oh she too good. Yeah. So no liking. Yeah. So it's still not a real Waichman.
A here is one standing in front of you. So the right hand downwards is in most, right. I ended people the most restricted. Yeah, because it's the internal rotation usually. So in me, the difference between my fingertips and here and there is probably about that long. And you have that actually quite often so you're not too liking here. But in a pill artist class that's as good as you get. So if you have one and a half handlings you would get one point here, stay here.
So no waking point yet. So the more working points you get, the stiffer you are and the more likely you are on the Viking constitution as a general tendency. The other thing is in sitting, if you're sitting next to me you are trying to rotate your whole body, including your nose to the side and if, and she can look way beyond but some people cannot even go 90 degrees to the side. So we are talking about some, think about some 80 year old man that are coming to your class. They are usually coming not to Pilatos classes for reasons that you can now understand that they cannot do the basic things, but you see them sitting in the pub, you see them in the, in the, in the cars outside, they are part of society and if you want to help them you better understand their constitution. So if you cannot go 90 degrees, no matter to which side, then you would get a second where I can point still no, why can point for you. But for me, let me see, I get 90 degrees here. Okay. No one I know. So I got to show it so far I, I was so worn with, so one viking point for me, but I failed in the second test here. The third test. So you have an upper hand and a lower hand and you try to extend such by using your powers, reaching upwards with the nose that you two hand separate as much as possible.
And then you see how much movement do you have between the hands and in you. This is about that much movement that you have there. So if you would not be able to separate more than one hand, which then you would get another waking point. So again, you're too flexible. Too much [inaudible] probably. Yeah. Okay. So then, uh, if you reach forward like you do here, the same test as we did before. Again, no Pelaton a no point for you.
But I have been working hard now. Now I can almost reach the ground with straight legs. But there are many people out there where the distance between the finger points and the floor is more than one handling their hand. Handlings this there all the more coming you have that. So that would be another viking point.
And the last one finally is if you sit on the ground, I'll do it together with you and you see how wide can you spread your legs no matter how you arrange your powers. This is wonderful here. Yeah. But there are many people who cannot go more than 45 or 50 degrees and they are usually in the last row of your classes, not in the front row there. And this is a genetic constitution that you see. It's not just here, it's, it's everywhere in their body. So that would be the last of the are the second to last Viking test.
So again, no viking point for you, but for me, no, this is more than 50 degrees now I can point for. Okay. And the last one is can you get your chin, no, your forehead and your need together at least on one side. So there are people who cannot do it on the right side because they have an injury. There are pain condition, but if you cannot do it on any site, then you're probably a viking person in general. So this is how the test would be performed. If you then give yourself all these points we need to bring in age and gender.
We didn't need to do that because a, if you have that restriction in a 90 year old man, it's unfair to apply the same conditions to him then to a 15 year old, a woman or historical. So you need to put in bonus points for gender and for age. And only then can you say, do you have the genetic constitution of a Viking personality? And then of course you will treat them very different. We have a third typology. Maybe for time reasons, I will only show it here. Okay. Okay. So maybe, so maybe we'll, we'll, we'll do it together.
And that is based on the teachings of Lardini or Yonda. And he described certain features in our sedentary culture, how people have certain joints, certain regions in their body where they are tight and other regions where they are soft. And you will find that in the literature. Most common is the upper cross syndrome in which they have tight chest muscles and also tight post here, your neck muscles here. But the front of the neck is very soft, very weak. And also the poster, your shoulder blade stable stabilizers are very weak.
So that's called the upper cross syndrome. Very common in people who don't do Pilatos who are just riding cars and sitting at desks. And you also have also quite common a lower cross syndrome in via in which the hip flexors are tight and the lumber erectors, but the abdominals and the gluteus maximus, they tend to be weak, quite common. Uh, he also described later what he called a layer syndrome that basically includes everything I just described from the upper cross in lower cross syndrome. But that included tight hamstrings. But it's the same thing that you have a tightness in one area that's complimented, supported in part by a weakness in another area.
And just working on the weakness alone is not sufficient as much as working on the tightness alone is not sufficient. You should address the whole pattern, very convincing. So what we have done is we looked in the literature and also experimented ourself whether we can develop a test for a crossover or Yonda topology. And this is out of [inaudible] new book in which he has described these regions of upper cross lower syndrome and of the layers syndrome together. So these would be the short and tight muscles here in the lightish glue. And here in the violet you would have the weak and the flacid muscles.
So now let's do the test.
Chapter 9
Crossover Test
It starts with the Chin to chest test. So you try to get your Chin as close as possible towards your chest and see how many fingers 10 you put together. Very nice. So this is one in our fingers you can put together if the minimal distance here is two fingers or more. Now you are not restricted enough. Yeah.
So because he can get closer than two fingers there. So if your, so you test for movement restrictions here. If you can get less than two fingers distance. If you can touch on you one finger or one an hour thing or like in you, then you don't get a under point for this one because you don't. Yeah. Even then, actually, Eh, you should be doing the test this out pain for this one.
So let's see how far you can go without see if, if you can stick one thing. Yeah, it's still less than two fingers. Yeah. So, so you can doubt maybe half a point that actually no, we made this in such a way that if you have a very clear answer, you would get two points. But in you, you have a debatable answer. So we would give you one point. Same for you. So if you are very, very clearly have an outcome where you say, I cannot do it, then you get two points. But if you can do it with cheating and with pain, then you get one point. And if you cannot do it Siro so, okay, so that's the first test. The second test is the knee to wall test where we test for possible movement restrictions on the posterior calf that you have a year. And let me take an artificial walls, all this so we can see it here.
If you go forward with your right foot, very nice that you touch it with the knee and also with the toes. And then you slide back half an inch at a time. How far can you slide back? As long as you heal can stay on the ground and the knee stays on the wall. Yeah, certainly my niece slides.
That's g no, but a you are here should stay on the ground. So if you would go but that's fine. That's fine. Yeah. So when does he'll leave the ground. That is a question. Yup. Yup, Yup. So you see here already you are having the habit, we having difficulties there and if you look down, this is not one hand links, this one hand, which there are people who can go much further back. So you get one young appoint for that. Because you have that restrictions, you cannot get further. So actually two points for this because it's a clear science.
Uh, now the better the better leg would be it. So if you do it there, so if even the air, because if you have an injury, uh, then the injury would be not your genetic constitution, but if even on the best leg you would be not better than this, then you get to younger points. So we should have done it on both legs and even on the best leg. Uh, you cannot get further away with the foot than one hand woods. Then you have a clear restriction in this part of the body and that would be congruent with [inaudible] cross over pattern. Let's go on a, the resting angel test.
I'll describe it first and then we see how we can demonstrate that here. Uh, here you're lying the back and with your arms to both sides, we see elbows resting on the floor and then slowly your slide along the floor, your arms upwards until the elbow can no longer stay on the ground. And again, you take the better side. And, and if you can get up to 45 degrees but not further with the elbow on the ground, even on the best leg, then you have a specific restriction that is congruent with the under test. Okay. So we start with those upper arms in one line and the elbow is touching the ground. And then you slide the arms are births as fine as you can go visit elbows in touch with the ground. Sure you're not cheating back here.
So if necessary, you maybe better to get the knees up. If you observe that you are trying to cheat here, which is happening in some people earlier than in others. And you can go much beyond 45 degrees and bows of your elbows are staying on the ground. So here they are starting to leave the ground. Some people again get all the way up. Yeah and but here it would start to leave.
But you're better than 45 degrees so you don't get the younger poets, you still have room to improve, but you don't fit perfectly into the topology. So again, if on the better arm you can only go 45 degrees but not further, then you have this specific restrictions and you would get the points for this one. And again everybody, the older Yom and the more likely you have some injuries. So we take the battle side because we are not interested in knee injury. We want to see if there is a general tendency in you in there. Now I can use you value on the ground also for the last test, which is the hip extension test. So here, let me show you on the picture first you are lying prone on your belly and you try to lift the right knee as far as possible backwards until or only as far as you do not go in a lot of those here. So that's where your right hand is here.
So you so, so you're trying not to tell your pelvis, see how far you can lift here. So this is a combination of weakness in muscles but also restrictions on the hip flexors in the front and pain there. Yeah. So we also need to see which leg is better. And the question is how, how many inches can you lift the battle knee off the ground. So here you have about three inches, four inches, or is it one hand lengths with, so as we can see in you, probably because of the pain is three.
Yeah. So you get two points. Yeah, you have a restrictions so you are very free in your shoulders but you fit into the lower cross syndrome, uh, in the under points and you partially fit into the car for restriction that you had there. So the lower cross model would fit for you. So the under description is actually quite helpful. So thank you very much for doing the tests with me. So let me round this up. Uh,
Chapter 10
How to Train Each Body Type
we have to develop this cross over point test. And uh, if you have, for example, six to eight point, then having a therapist who focuses particularly on these restrictions will be very helpful. I made a slight difference. A slight mistake in my description. This is not so much genetic constitution.
This is your life habits speaking to you. It's decades of sitting, of not doing gymnastics, et cetera. So I don't think it's genetics, it's being homo-sapiens in the 21st century and then having, having all these front lawyer and station, not so much reaching backwards and uh, and uh, non species appropriate movement environment that has found its way creeping into your body into this specific areas of shortening. So here in the hip you had that and here, but up here you did something very nice in your life and probably not yours, your genetic constitution, it's your active movement prep artwork that you have been using better up here than down here. Ah, okay. Yeah, so that makes sense. Okay.
So then you would work very different with each of these types. Um, for time reasons I think I'll just go through them point by point. If you have a why king, you would load the Fascia in the end load position and I'll show you a brief example for that so that the tissue gets long in the end load position. You would also do final exhaustion, for example in the regime, not in the short position. So you would do the last repetitions in the long position and then take a break.
That would be very different. If you are Bendy Wendy, then you would do the last repetitions of a movement in the shore position. So then the terror ban, the elastic bands have no use for why king because they have little resistance in the long position but have maximal condition in short position. But for Ben, the Wendy getting the therabands is ideal because they train your muscle where you want to put the emphasis of the load, which is in the short position. Interestingly enough also for the Viking, you would do super slow foam roller Rees self treatments because you want to break down collagen sentences. Whereas for the Benu Randy, for the temple dancer, you would do more vigorous stimulation because you want to increase collagen production. For the Viking, you would teach a more body friendly attitude. Listening to the body robot is not a victim. Be more friendly. With the Bendy Wendy, you will teach them stability.
You know that they cause stability would be very important for them to learn. Eh, you can now put that in the weight gym that we have been doing where you, if they have a regime, uh, environment already, it's easy for them to exercise their, uh, these are the general principles that we have developed where you start with the 10 Segal, uh, expansion. So we are now working on a facial muscle training on federal strengths training and that would be in general whether you're bendy, Wendy or viking, you would have these five steps in a year preparatory counter movement. We covered that in their fascist science lecture. That's on politeness. Any time you would have proximal initiation and then the distal delay and you would have mini bounces in both and position with the weight, of course not with the maximum rate.
Now this is now how we round this lecture up for the Viking who has high pole mobile joints. So lacking enough mobility, you would do the mini bounces and the long position here, not down here where you have that weight. Um, and you would do the final exhaustion where he does the long in the long position. Whereas for the Bendy, Wendy, you will be doing it different. You would do in the short position that would be down here, but with bench press it would be here. So where the muscle is in the shortest position there you would do active, uh, alive, short bounces to stimulate the fibroblasts and you would do your last repetitions in the short range because then you develop more sarcomeres in the muscle. So you, the muscle gets long. Or in terms of its architecture for their Benny Randy's, your research has shown that they have appropriate separative deficit, particularly in the long range position through should include that not as strengthening exercise but as refinement. So they should go in the long range, could position but without maximum load.
And more looking at how refined, how precise, how slow, how jerky less, how smooth. Can you do the movement there? Okay. To finish up the lecturer, if you like to learn more about Fascia, uh, I highly recommend our summer school that we are doing every two years. It's a one week long experience to dive into Fascia. We have a fashional net as a a rep site to look for books, DVDs, et Cetera.
And every three years we now have a congress connective tissues in sports medicine at all university. Ah, it's in 2016 here. Thank you. So the summer school is September for the ninth 2016 and then it will be again two years afterwards. And the most strongest recommendation is consider what we do. Become a member of the Fascia Research Society there you get reductions to almost everything here and you get the number one journal to be informed or new insights in the field of fashion related therapy and fashion research, which is the Journal of Bodywork and movement therapy.
And finally, last slide. If you like Fascia, please do it on a non high horse. Don't go out with an arrogant attitude that you know everything better and everybody else is stupid. That is the style in the fitness culture. How you have people think you are great and you think you are great. But I think it's much better to be humble. Fascia has been neglected in the past in health oriented movement.
People have been looking at muscle training at coordination, at cardiovascular training and connective tissue had been considered to be useless. So and now thanks to the research and many other people involved, the daughter is back in the family and she was declared to be tested and stupid or inert and not to alive or whatever. And now she is part back, but she's not the biggest player. Uh, if you would only attend to the daughter, that would be not appropriate, but please include her in your cardiovascular training, in your muscle training, in your coordination training. And I think that is the appropriate place. And thank you very much.
Chapter 11
Q&A
Part of chronic fatigue syndrome and FIBROMYALGIA is sleep disruption. Yeah. So I, it hit me then, whether the sleep disruption comes first and that then triggers the physiological pain and extreme stiffness. I mean, it's something I've dealt with a lot earlier in my life and I would bend over, you know, like just stretch my hamstrings that forward bend. I could get there, but then to come back up, I, there was no elasticy it, I w it would be so stiff to get back up and then it would take me a few minutes to recover, you know, back up. So really what it felt like is that it would stretch, but there was no rebound and that seemed to be the hallmark of the fibromyalgia texture and whether the lack of sleep is what then triggers the connective tissue.
So that's why professionals who are treating chronic fatigue and fibromyalgia, they often mix but not always, but they have a lot of similarities, uh, that they say under certain conditions if lack of sleep, it's really highly developed. You need to treat that even with chemicals, sleep medicine that may have side effects, but that's still a better solution that we get you to get some rest for a few nights before our nutrition, before our Fascia therapy, before our offing treatments, et Cetera can have any effect. That's not a longterm solution to have sleeping pills all the time, but at a certain stage those professionals who are treating fibromyalgia, there are many clinics who had been focusing on that. They say that may be a necessary requirement, not a sufficient requirement towards getting the whole chicken and egg soup in a positive spiral direction rather than in a negative spiral direction. Yes, I agree by my very well [inaudible]
I'm on there. Oh, I didn't know that. So you do boxing clubs for Parkinson, right? Yeah. Yeah. Interesting. Because that is very challenging. So people are sweating and I hyper active. It's more factual that she was recommended to workout hard. Yeah. Two hours at a time. Okay.
Two or three hours a week cause she's got pretty extreme. She didn't come to Kathy for a long time. Um, she's removed Parkinson's. Yeah. But so even she won't quit. I mean she's so committed to her two hours session. Okay. Two hours is a lot. Yes. [inaudible] this is good in the way CIM, if people are doing weights and muscle strengthening, they say they should pause one minute between the sets and then you get the growth hormone up. If you are men who want to have more testosterone, then you pause only for 30 seconds between the sets.
So as we age, we have more and more waste products in the water of our ground, substance free radicals that are part of aging but also of stressful living. And then using the foam rollers is a very nice way to push the old stagnant water out and to get fresh water into it. But doing stretching is also a sponging effect. Yeah. And Movement. Yeah. And, and also increasing the microcirculation. So if you do both, the circulation alone, the image of the river in the desert is not sufficient. But if you make the land thirsty and then you will increase the circulation, the water needs to go there. Why are the little outer y'alls?
It doesn't go there by drinking alone.
So then the circulation is active and you make sure that that the freshwater gets in all the old dry pockets that you have there. So it would be good. Yeah.
And yet on the other side you have somebody who's very mobile and very flexible and sort of the cold in the condensing, in the feeling of compacting, maybe doing like cryotherapy and things like that. I'm just wondering how, how much of that is just sort of a bandaid on top of the issue and how much is maybe allowing their body to have a sense of the opposite and open the
The good thing on warm air is it also makes the muscles more action ready. So if you needed the muscles to protect yourself from hybrid extension tension, they are more ready. So warms makes the red muscle fibers weaker. If you try to swim in cold water, you will see you have less ATP turnover, but it makes it college and softer. On the other side, if you are bendy when the person under warm condition, you would go also go much further. Uh, but for example, the, in cold conditions you would have a little bit more stability in there. So this is quite interesting how how you use warms for different, uh, conditions. Uh, the warms also has an inflect on the inflammation.
So if you have inflamed conditions, you would not like to have warms immediately afterwards. Then people apply cold. That shorten say inflammation phase. But that could be good or bad because if you shorten the inflammatory wound healing phase, you are, you recover faster. You can be back on the soccer field earlier and continued training for example, or becoming a hero.
But the ultimate repair of the tendon is not so good. So, uh, if you leave the inflammation in there, unless it's a chronic inflammation, but if you leave the natural healing cycle, this is a pain. So if you take a ensades non-steroid antiinflammatory drugs, you also shorten the inflammatory wound healing phase. You have less pain, which is good, but the ultimate strengths of the Achilles tendon is weaker. So that would be also the disadvantage of applying cold treatment after athletic performance. Uh, the, your reinjury rate could be higher, uh, because the Collagen hasn't completely regenerated after micro injury. So this again, good and bad sites in it
If these different layers and then how and when we use those different tools to help that overall picture. Yeah. Yeah.
So again, you need to look at the person and what are the advantages and the disadvantages of warms of coldness and of many other interventions. Good questions.

Workshops: Anatomy and Fascia
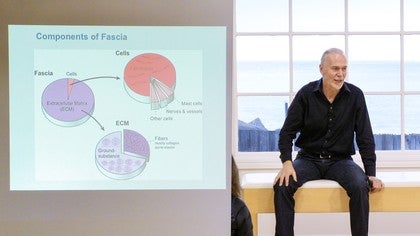


Mention
 |
Robert Schleip (Teacher) |
|
|
Aline B |
 |
Gia Calhoun |
|
|
Sara D |
 |
Rossana C |
 |
Lynn P |
|
|
Yunus E |
Comments








You need to be a subscriber to post a comment.
Please Log In or Create an Account to start your free trial.
